Join tribal leaders to learn about policy changes and other strategies that support the People and Land
Participants from the 2012 Our Food is Our Medicine Conference hold up vegetables cooked in a traditional pit oven. Photo courtesy of NWIC
Source: Ryan Key-Wynne, NWIC
Studies show that returning to a more traditional diet can help Native Americans improve health and reduce problems such as diabetes. People from throughout Indian Country have put those findings to work and are contributing to policy changes and strategies that promote access to traditional foods.
Many of these champions for traditional diets will gather at the second annual Our Food is Our Medicine conference, hosted by Northwest Indian College’s Institute of Indigenous Foods & Traditions. The conference brings together tribal leaders and allies, giving them opportunities to teach and learn from each other while initiating ongoing relationships that will benefit all.
“We are very excited to host this gathering, which brings people together to discuss successful models for activating policy change in tribal communities,” said Meghan McCormick, coordinator of the Institute of Indigenous Foods & Traditions, which is a program of NWIC’s Cooperative Extension Department. “While many tribal agencies throughout the United States engage in work related to wellness through traditional plants and foods, there is often little collaboration between these organizations. Most are burdened by incredibly heavy workloads. This gathering will be a platform for people to connect, share ideas, and inspire one another.”
One speaker who is sure to inspire at the conference is Micah McCarty (Makah), the former chairman of the Makah Nation and current chair of the First Stewards Board (among many other leadership roles). McCarty is one of the keynote speakers lined up for the conference. His work in Neah Bay, Washington led to significant headway in strengthening the response to oil spills in coastal waters, helped to protect tribal whaling rights, and fostered strong connections between tribal and non-tribal governments.
In addition to invigorating keynote speakers, the conference will include interactive workshops, plant walks, traditional food sharing, storytelling and cooking demonstrations.
“This year we are focusing on policy in support of the People and the Land,” McCormick. “We will be discussing strategies that will bring traditional foods in tribal programming and how to build partnerships with land holders to sustainably harvest and protect resources”
Some workshops will include:
Tribal Food Sovereignty Projects
Policy in Government Programs
Tribal Food Policy Council
Policy to Improve Access & Protection of Gathering Sites
GMOs
Seed Saving
Composting
Climate Change & Policy
Seaweed Demonstration
Activating your Story
The conference will take place Sept. 11-13 and will be held at Bastyr University, an innovative university focused on natural health education near Seattle, Wash. The registration cost for the conference is $200, day passes are $100.
For more information, contact Meghan McCormick, Institute of Indigenous Foods & Traditions coordinator, at (360) 594-4099 or mmccormick@nwic.edu. To register, visit bit.ly/ofom2013.
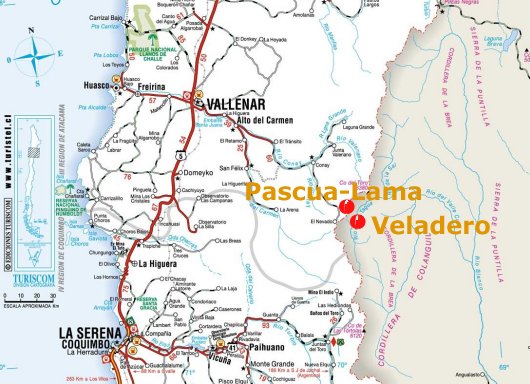
In this May 23, 2014 photo, a chicken carcass lies on top of a tank found by grape grower Pascual Abalos Godoy on his morning rounds, who believes the chicken died from drinking contaminated water, in El Corral, near the facilities of Barrick Gold Corp’s Pascua-Lama project in northern Chile. The residents living in the foothills of the Andes, where for as long as anyone can remember, have drunk straight from the glacier-fed river that irrigates their orchards and vineyards with clean water. Since the Barrick gold mine project moved in, residents claim the river levels have dropped, the water is murky in places and complain of health problems including cancerous growths and aching stomachs. (AP Photo/Jorge Saenz)
By Associated Press, Published: July 22
SANTIAGO, Chile — Chile’s Diaguita Indians are asking the country’s supreme court to require the world’s largest gold mining company to prepare a new environmental impact study for an $8.5 billion mine that straddles the mountaintop border with Argentina.
Attorney Lorenzo Soto filed the high court appeal Monday.
The Indians already won an appellate ruling that requires Barrick Gold Corp. to keep its previous environmental promises and says the watershed below the Pascua-Lama project is in “imminent danger.”
The Canadian company has publicly promised to do any work required.
But Soto says his 3,000 plaintiffs want Barrick to apply for a new permit that takes into account their anthropological and cultural claims to the watershed below the mine.
Barrick told The Associated Press it had no immediate comment on the court filing.
Copyright 2013 The Associated Press. All rights reserved. This material may not be published, broadcast, rewritten or redistributed.
On a cool spring morning in the mountains of southwest Washington, 12-year old Cathy Cahill helped her dad plant scientific instruments around the base of trembling Mount St. Helens. A few days later, the volcano blew up, smothering two of his four ash collectors. When he gathered the surviving equipment, Cathy’s father found a downwind sampler overflowing with ash laced with chlorine.
Cathy Cahill holds a carbon-fiber AeroVironment Raven she will use to sample plumes of hazy air. Photo by Ned Rozell
Tom Cahill of the University of California, Davis, wrote a paper on this surprising result; editors at the journal Science were impressed enough to publish it.
Tom’s teenage daughter was not a co-author on her dad’s Mount St. Helens paper in the early 1980s, but her name has appeared next to his in a few journals since then. Now 44, Cathy continues to stamp her own mark on the field of atmospheric science. The University of Alaska Fairbanks professor has captured and examined the particles floating in air breathed by U.S. servicemen and woman in far-off deserts. She has invented an air-sensing system that alerts pilots they are encountering volcanic ash particles. She also spoke on a national radio program about the bitter, smoky midwinter air of her adopted home of Fairbanks, Alaska.
And she now commands a fleet of 161 unmanned aerial vehicles. Cahill will fly 160 AeroVironment Ravens (which have a wingspan, at 55-inches, more like a sandhill crane’s) and one Boeing Insitu ScanEagle (which weighs 10 times more and has the 10-foot spread of a California condor). She will use them to sniff the air around volcanoes and inside wildfire plumes.
Cahill will also enlist the drones to expand her ground-based studies of air from Afghanistan, Djibouti, Kuwait and other regions in which Americans are stationed. For years, she has helped officials with the U.S. Army Research Lab see the tiny particulates wafting in the air above urban battlefields.
“The military has a healthy population, but we’re still seeing increases in respiratory diseases in soldiers that are coming home,” she says in her office that overlooks the flats of the Tanana River valley, home to both an Army post and an Air Force base. “They call it ‘the Iraq crud’ — you come back hacking. We’re trying to find out what might be responsible for some of these respiratory ailments.”
Along with the health of men and women, military officials have also asked Cahill what particulates are doing to their machines.
“A lot of soils behave like volcanic ash,” Cahill says. “That’s part of the reason engines tend to get destroyed in Saudi Arabia. The soils there can melt in the engines. And soils in high enough concentrations also abrade. If you have high concentrations and you fly through them again and again, you’re going to wear out your aircraft.”
Geophysical Institute machinist Greg Shipman and an electronics specialist, David Giesel with the unmanned aircraft program, helped Cahill convert her ground-based air samplers from a 40-pound Pelican case to an eight-pound unit that fits in the nose of an unmanned aircraft. Her air samplers will lead the way into volcanic ash clouds and choking plumes of singed black spruce.
Going airborne is just another step in the life of the little girl who followed her father’s footsteps over a volcano many years ago.
“My entire career’s thread is aerosols — the sources, atmospheric transformations, transport and impacts,” she says. “If you’re studying the atmosphere, you want to be able to go up in it.”
Since the late 1970s, the University of Alaska Fairbanks’ Geophysical Institute has provided this column free in cooperation with the UAF research community. Ned Rozell is a science writer for the Geophysical Institute
Coca-Cola sales are plummeting in the wake of a growing movement away from sugary soft drinks in the U.S. and increasing concerns over the link between sugar, obesity and diabetes.
Profits for the global soda giant dropped by 4 percent this quarter, compared to last year at this time. The overall drop was influenced by a total soda sale decline of 4 percent in North America, where consumers are caught in the midst of a battle between retail advertising and government warnings over the negative health impacts of soda.
In June, the American Medical Association labeled obesity a disease, pointing a finger directly at the increase of U.S. sugar consumption and calling on the United States Department of Agriculture to cut sugary drinks out of government-sponsored food assistance programs.
The call to cut back Americans’ intake of sugar comes after New York City Mayor Michael Bloomberg’s soda ban, a proposal that would have banned sale of sugary drinks — mainly sodas — that come in containers larger than 16 ounces. While the proposal is still being worked out in the courts, the Bloomberg’s proposal brought the debate about soda’s health impact to the front lines.
Coca-Cola isn’t pointing to the social debate over sugary drinks as the main component of its decline in sales. Instead, it’s talking about the weather.
“Our second quarter volume results came in below expectations, reflecting an ongoing challenging global macroeconomic environment and unusually poor weather conditions in the quarter,” Coca-Cola CEO Muhtar Kent said in a press release following the second-quarter earnings release.
While Coca-Cola claims its downturn in North American soda sales is largely due to weather, arguing that people drink fewer sugary beverages when it’s just not nice out, it comes in the midst of a U.S. health-inspired trend that’s moving consumers away from the sugar-filled drinks that make up the company’s portfolio.
“Soft drinks are the devil product at the moment,” London Metropolitan University nutrition policy professor Jack Winkler told the Wall Street Journal.
Coca-Cola denial and the growing scientific debate
In an attempt to stay relevant in the midst of a society growing more aware of the impacts sugary drinks have on health, Coca-Cola is in the midst of attempting to create a soda that uses low-calorie sweetener while still providing a full-body taste.
This follows a campaign launched at the beginning of the year that attempted to brush off the obesity scare, urging Americans instead to get out, exercise and quench their thirst with a Coke product.
“We’re watching, we’re learning,” Steve Cahillane, who heads Coca-Cola’s North American division told CBS News.
The company is also engaging in the nationwide conversation, portraying itself as a leader in the fight against obesity. A commercial released recently aims to market Coca-Cola as a company intent on reducing calorie consumption and battling the obesity epidemic.
According to the American Medical Association, 36 percent of American adults are obese or overweight. If trends continue, experts predict that could rise to 50 percent of Americans by 2040.
On top of obesity, the nation is also seeing a rise in Type 2 diabetes. A recent Harvard study indicated that people who drank two cans of sugary drinks a day had a 26 percent greater risk of developing diabetes. It also found that men and women who increased sugar consumption with a 12-ounce serving per day gained an average of 4 pounds every year.
“For over 125 years, we’ve been bringing people together. Today we’d like to come together on something that concerns all of us: obesity,” the Coca-Cola commercial states. “The long-term health of our families and the country is at stake. And as the nation’s leading beverage company, we can play an important role.”
The commercial goes on to give a glowing report of just how hard Coca-Cola is working to provide “healthier options” for American consumers, claiming that a growing percentage of products are ones that have been severely limited in caloric content.
“Across our portfolio of more than 650 beverages, we now offer 180 low- and no-calorie choices and most of our full-calorie choices now have low or no calorie versions,” the ad states. “Over the last 15 years, this has helped reduce calories per serving across our industry’s products in the U.S. by about 22 percent.”
Will Coca-Cola win the ‘health’ battle?
By the end of 2013, Coca-Cola plans to help limit portion sizes by offering smaller bottles and cans of various sodas available in 90 percent of the country, according to the advertisement. This adds to what it claims are efforts to help consumers make the right choices.
The commercial states that elementary and high schools throughout the nation have been equipped with Coca-Cola vending machines that have increased the choice of low- and no-calorie drinks, including diet sodas.
According to a Wall Street Journal report in March, one-third of North American Coca-Cola sales came from low- and no-calorie beverages.
“We are committed to bring people together to help fight obesity,” Stuart Kronauge, Coke’s North America Sparkling Beverages Division general manager told Time magazine. “This is about the health and happiness of everyone who buys our products and wants great-tasting beverages, choices and information. The Coca-Cola Company has an important role in this fight.”
In line with Coca-Cola’s push for no-calorie drinks in U.S. schools, a study published in the American Journal of Clinical Nutrition indicates that from 2007 to 2008, 12.5 percent of children were consuming artificially sweetened beverages during a 24-hour time period — double the amount children were drinking 10 years ago.
And while that gives the company a favorable statistic in terms of sugar content, with a 90 percent reduction in beverage calories sold in U.S. middle and high schools since 2004, it doesn’t eliminate health concerns.
Concerns over the no-calorie push
A mock Coca-Cola anti-obesity advertisement addresses this issue, citing health concerns related to the use of no-calorie sweeteners.
“Even though we’ve reduced the calories per serving, these beverages can still cause kidney problems, obesity, metabolic syndromes, cell damage and rotting teeth, which leaves 470 beverages which have extremely high unhealthy levels of calories,” the mock ad states.
The ad that took a stab against Coca-Cola is based on studies conducted on aspartame, the ingredient that is most often found as a substitute for sugar in low- and no-calorie beverages.
It wasn’t too long ago when no-calorie sweeteners were considered dangerous chemicals.
In 1958, Congress required the FDA to ban any additive that was known to cause cancer in animals or humans. In the 1960s, cyclamate was removed from U.S.-sold products when it was linked to cancer. Specifically, chicken embryos that were exposed to aspartame began to develop deformities. A later study showed rats fed the product grew bladder tumors, according to a Time magazine report.
By the 1980s, aspartame moved on to the market, becoming the preferred additive for diet colas. This was after a 1980 Food and Drug Administration Board of Inquiry study that initially deemed the additive to be potentially dangerous and a carcinogen.
“The Board has not been presented with proof of a reasonable certainty that aspartame is safe for use as a food additive under its intended condition of use,” the report states.
However, a year later a new set of studies favorable to aspartame emerged, and it was approved for U.S. market consumption.
In 1985, Monsanto purchased G.D. Searle, the company that owned the aspartame patent. Since then, it has become the go-to for the soda companies, including Coca-Cola in their quest to produce low- and no-calorie beverages not just throughout the U.S., but throughout the global market.
“The key here is to ensure that in every market where we operate to have no- or low-calorie beverages of our main brands available,” Kent said in a conference call, according to the Wall Street Journal. “We do not have that consistently across the world today.”
Mark Mulligan / The Herald Sandy Swanson, a licensed practical nurse at the Tulalip Health Clinic, waters plants in the new garden outside of the clinic on June 16. Swanson works in the elder care program, and when she gets a chance will duck outside to work in the garden. “It makes me smile to come out here and care for these plants,” said Swanson.
By Bill Sheets, The Herald
TULALIP — When a doctor at the Tulalip tribal health clinic advises a patient to eat healthier food, it doesn’t have to be only words that are heard or written down on paper.
The doctor can take the patient right outside the building and show them that they can grow that food for themselves.
A small, rudimentary vegetable garden at the Tulalip Karen I. Fryberg Health Clinic was greatly expanded this year with several new raised wooden beds. Leeks, kale, squash, cucumbers, peas, tomatoes and more are thriving in their southwestern exposure to the summer sun over Tulalip Bay.
Culinary and medicinal herbs and plants are being grown as well — parsley, tarragon, basil, lavender and rose hips, to name a few.
“It’s about engaging with our patients,” said Bryan Cooper, clinical lead at the health center. “Instead of telling them what to do, it’s ‘Let’s work together.'”
The incidence of diabetes on the reservation is high, and the garden is especially geared toward helping diabetics manage their condition through their diet.
Doctors and staff members from the lab and pharmacy have been accompanying patients to the garden to discuss the possibilities, said Roni Leahy, diabetes coordinator at the clinic.
Planting soil, tubs, gardening materials and advice have been dispensed on special-event days at the clinic, such as a recent “Diabetes Day.”
In one program there, young people have been taught traditional ways of harvesting and processing native medicinal plants. In another, titled “Gardening Together as Families,” a popular community vegetable garden was established.
At the clinic, the idea was to build on the success of the Hibulb programs and create a direct link between the medical facility and healthy diets, staff members said.
The late Hank Gobin, the tribes’ cultural director who helped establish the Hibulb programs, was motivated to improve tribal members’ diets in part because he himself was a diabetic. He passed away in April at age 71.
“It’s always about people and their health and well-being,” Leahy said. “That’s how we keep his memory alive.”
The clinic garden has been maintained by staff members and volunteers. At the end of the season, the food will be used at tribal events, Leahy said.
Sandra Swanson, 73, a career nurse, works full time in the clinic’s elder care program.
“Then I come out here and play,” she said, as she dug in one of the planters.
The plan is to expand the garden next year to a nearby slope facing the bay, with terraces and a trail, Cooper said.
More volunteers are needed, staff members said.
“We want to start these (gardens) and get them to a place where the community takes over,” Cooper said.
Bill Sheets: 425-339-3439; sheets@heraldnet.com.
Health fair
A health fair and blood drive is scheduled for 9 a.m. to 3 p.m. Friday at the Tulalip Karen I. Fryberg Health Clinic, 7520 Totem Beach Road.
Is your child up to date? Vaccines required for school are available to children at no cost
Source: Snohomish Health District
SNOHOMISH COUNTY, Wash. –– More 5 and 6 year olds in Snohomish County had all the vaccines they needed to enter school last year, according to recent data released by the state Department of Health. For the 2012-2013 school year, 86.3 percent of local kindergarteners were up to date on their shots, better than past years and higher than the state average of 85.6 percent
Vaccines are required for school children because they prevent disease in a community setting. The rate of vaccination has continued to climb since an all-time low in 2008-2009
School districts report vaccination rates to the state. The highest immunization rates for all grades (K-12) in Snohomish County last school year were in Lakewood (94.8%) and Everett (94.7%) school districts.
A small percentage of families seek exemption from the vaccination requirement, an average of 5.3 percent in Snohomish County schools compared to 4.5 percent statewide for children entering kindergarten.
In 2011 the process for parents or guardians to exempt their child from school or child care immunization requirements was changed. Parents need to see a medical provider to get a signature on the Certificate of Exemption form for their child’s school. More information about the form and the law is available online at www.doh.wa.gov/cfh/Immunize.
Although exemptions are allowed for medical, religious, or personal reasons, the best disease protection is to make sure children have all their recommended immunizations. Children may be sent home from school, preschool, or child care during outbreaks of diseases if they have not been immunized.
Summer is a good time to make sure your children are up to date on required shots. The cost of childhood vaccines is subsidized by federal and state government so that every parent can choose to have their child protected without regard to cost.
Required childhood vaccines are available for the school year 2013-2014.
· Two doses of chickenpox (varicella) vaccine or doctor-verified history of disease is required for age kindergarten through grade 5. Students in grade 6 are required to have one dose of varicella or parental history of disease.
· The whooping cough (pertussis) vaccine, Tdap, is required for students in grades 6-12 who are 11 years and older.
Recommended vaccines also are available.
· Varicella vaccine for children in grades 7-12 who have never had chickenpox.
· Meningococcal vaccine for adolescents age 11-12. A second (booster) dose at age 16-18 if first dose was given at ages 11-15.
· A three-shot series of human papillomavirus (HPV) for both adolescent boys and girls age 11 and older.
· Children 12 months and older should receive hepatitis A vaccine, a two-shot series.
· Flu vaccine for all people age 6 months and older.
Snohomish Health District promotes routine vaccination of children and adults.
Snohomish Health District’s Immunization Clinic will serve you if your family does not have a health care provider. A visit to a Health District clinic includes a check of your child’s record in the Washington Immunization Information System, the state’s immunization registry.
Parents should beat the rush by making appointments now with their child’s health care provider. At the Health District, parents can make an appointment during normal clinic hours at either the Lynnwood or Everett office.
A parent or legal guardian must accompany a child to the clinic, and must bring a complete record of the child’s immunizations. You need to fill out a Snohomish Health District authorization form to have another person bring your child to the clinic. Ask the clinic staff to mail or fax a form to you.
Health District clinics request payment on the day of service in cash, check, debit, or credit card. Medical coupons are accepted, but private insurance is not. The cost can include an office visit fee, plus an administration fee per vaccine. Reduced fees are available by filling out a request based on household size and income.
Teens also occasionally require travel vaccines for out-of-country mission work or community service. The Health District offers those immunizations and health advice for traveling in foreign countries.
Please call if you have questions, concerns or to schedule an appointment: SHD Immunization Clinic 425.339.5220.
Read more about the state’s vaccine requirements for school-age children and child care. Find more information about Washington’s school immunization data.
Established in 1959, the Snohomish Health District works for a safer and healthier community through disease
prevention, health promotion, and protection from environmental threats. Find more information about the Health District at www.snohd.org.
Back-to-school shots hours:
SHD Everett Immunization Clinic, 3020 Rucker Ave, Suite 108, Everett, WA 98201
425.339.5220
By appointment: 8 a.m.-noon and 1-4 p.m. Monday-Wednesday-Friday
Announcement of a Tuberculosis (TB) History Project in Snohomish County
The TB Voices Project for Snohomish County is looking for persons to share their tuberculosis (TB) stories with the community. Whether you or a loved one had TB, your story is important. Share your story on our website or contact us for a recorded interview.
The purpose of the TB Voices Project is to allow individuals from all generations throughout the county to tell their TB story, and in turn, these stories can help persons around the globe currently impacted by TB.
For more information go to www.Tbphotovoice.org or contact Project Director, Teresa Rugg at 360.862.9034, twrugg@frontier.com.
The TB Voices Project for Snohomish and King County is a project of TB Photovoice, in partnership with the Firland Foundation. Since 2006, TB Photovoice (based in Snohomish) has worked around the world to amplify the voices of individuals directly impacted by TB so that they, as well as their communities, can improve their overall health.
A resolution in support of the Public Health and Safety Code of the San Carlos Apache Tribe (SCAT) has passed that will directly impact the lives of Natives living with HIV/AIDS. According to SCAT HIV/AIDS Coalition Chair and Public Health Emergency Preparedness Coordinator Anita L. Brock, this resolution should help curtail the spread of communicable infectious diseases such as HIV/AIDS. It offers tribal members “the system needed to continuously address the threat such diseases pose to the San Carlos Apache community,” Brock says. “The implementation of such a Code supports enforcement of public health responsibilities and the authority needed to identify the risk factors associated with the spread of infectious disease.”
According to HIV/AIDS activist Isadore Boni, a SCAT member and key supporter of the resolution, passage of this resolution does much more: “HIV/AIDS confidentiality is now in our health codes.”
Boni explains that this resolution “allows the protection and confidentiality of public health information and patient privacy, especially for those who have been infected by HIV/AIDS.” Another key component of this resolution, according to Boni, is that it renders HIV testing optional for SCAT members. “There was talk of doing mandatory testing,” he says, “but I advocated against it.”
According to Brock, who worked with the primary team in development of the code now in place, this new resolution benefits not just enrolled SCAT members, but Natives throughout Indian country. “The code adds to the infrastructure needed to make decisions that will benefit all tribal members,” she explains. “They will be the benefactors of a system which values their privacy and continuity of care. In addition, Indian country is quite vast with over 500 tribes, and each tribe may make this determination. From a purely public health perspective, the benefits are self-evident.”
The Centers for Disease Control (CDC) reports that American Indians and Alaska Natives ranked fifth in rates of HIV infection in 2011, “with lower rates than blacks/African Americans, Hispanics/Latinos, Native Hawaiians/Other Pacific Islanders, and people reporting multiple races, but higher rates than Asians and whites.” However, American Indians and Alaska Natives have poorer survival rates than all other ethnicities and races.
Boni believes the official CDC numbers documenting the rates of HIV infection among Natives may be significantly lower than the actual rates of HIV/AIDS throughout Indian country.
“I personally know more people on my reservation that have HIV than what our Indian Health Service has in San Carlos,” Boni claims. “People like me get tested in the city, so our numbers do not get counted, and agencies and even tribes do not share information. So how many people actually have HIV/AIDS? No one really knows.”
Boni was diagnosed with HIV and Hepatitis C in 2002. He relocated to Phoenix, Arizona for treatment. “There was, and still are, no services for tribal members who are HIV positive on the reservation.” He says he was homeless in Phoenix for two years and lived on the streets, in halfway houses, and in shelters. He was beaten, and his medications were stolen. He worked as a laborer making minimum wage by day, to try to put together funds to pay for shelter and food at night. On World AIDS Day in 2004, Boni shared his story for the first time, and he has been a public advocate supporting the lives of HIV positive Natives ever since.
“Confidentiality has always been a problem on my reservation,” Boni says. “Many people have shared with me that their health information was disclosed without their consent.”
Boni, who has a bachelor’s degree in social work from Arizona State University, goes on to say that privacy rules and regulations had not been in practice in San Carlos. “It got to a boiling point for me. I assertively pushed the San Carlos Health Department to do something about this.”
Partly due to his efforts, the resolution passed in time for National HIV Testing Day, in June of this year. “HIV disclosure is painful, not only for the individual but their families,” Boni explains. This new code protects them.
“I know the decision-makers in our health department are still clueless as to the impact HIV/AIDS has on our reservation,” Boni continues. “To them it’s not a priority, but I remind them over and over that this health crisis is serious. No San Carlos Apache tribal member should have to die of AIDS complications in order to prove that this is a problem. Period.”
Since genetically engineered foods were introduced in 1996, the United States has experienced as upsurge in low birth-weight babies, infertility and an increase in cancer.
Agricultural tech giants like Monsanto have restricted independent research on their crops, which is legal, because under U.S. law, genetically engineered crops are patentable. The studies that have been conducted link genetically modified foods to a vast array of diseases—and long-term effects have yet to be measured.
Below, Indian Country Today Media Network rounds up the five most deadly genetically modified crops or substances on the market that you should avoid at all cost.
1. Corn
This is not our ancestors’ corn. Genetically modified corn contains toxic materials and is at least 20 percent less nutritious for our bodies, according to a report titled “2012 Nutritional Analysis” by globalresearch.ca.
Corn is the worst offender on the GMO list, because at least 65 percent of the U.S. corn production is genetically modified, and it is found in so many products and forms—on the cob, in nearly every processed food with corn syrup, in the corn feed consumed by the chickens and cows you may eat, and the list goes on.
Genetically engineered corn contains the highly toxic gene Bt (Bacillus thuringiensis), which Monsanto introduced in the 1990s to make plants immune to Roundup, which is Monsanto’s weed and insect killer that tears into the stomachs of certain pests.
According to Sherbrooke University Hospital in Canada, Bt has been found in the blood of humans, including in 93 percent of pregnant women they tested, in 80 percent of the umbilical blood in their babies, and in 67 percent of non-pregnant women tested.
2. Soy
More than 90 percent of soybeans grown in the United States are genetically modified, and animal studies have shown devastating effects from genetically engineered soy, including allergies, sterility, birth defects, and offspring death rates up to five times higher than normal, according to Dr. Joseph Mercola in the Huffington Post.
Americans typically consume unfermented soy, mostly in the form of soymilk, tofu, TVP, and soy infant formula, which have at least 10 adverse effects on the body, like reducing one’s ability to assimilate essential nutrients and increasing the potential for thyroid cancer.
3. Sugar Beets
Sugar beets comprise more than 50 percent of U.S. sugar production, while sugar cane counts for the remainder, Natural News reports. Last year, the USDA deemed genetically modified sugar beets safe, de-regulating the crop. Now the hazards of an already toxic substance are exacerbated, presenting the likelihood of increased cancer rates, changes in major organs and the gastrointestinal tract, allergic reactions, infertility and accelerated aging.
But all sugar is best avoided, according to a specialist in pediatric hormone disorders and the leading expert in childhood obesity at the University of California School of Medicine in San Francisco, Robert Lustig. “Sugar is not just an empty calorie, its effect on us is much more insidious. It has nothing to do with the calories. It’s a poison by itself,” Lustig says.
4. Aspartame
This fake sugar substitute is made from genetically modified bacteria and is used in basically every diet soda and product on the market.
Aspartame “has been linked to a number of diseases, can impair the immune system, and is even known to cause cancer,” Natural News reported. In one study, of the 48 rats given aspartame, up to 67 percent of all female rats developed tumors roughly the size of golf balls or larger.
5. Canola
Canola—marketed as being void of “bad fats”—is a genetically engineered oil developed in Canada from the Rapeseed plant, which is part of the rape or mustard plant family.
Rapeseed oil is poisonous to insects and used as a repellent.
So while olive oil is made from olives and coconut oil is made from coconuts, canola oil is made from the rapeseed. Canola is short for “Canadian oil low acid.”
Agri-Alternatives, a magazine for the farming industry, notes “By nature, these rapeseed oils, which have long been used to produce oils for industrial purposes, are… toxic to humans and other animals.”
But, canola oil companies insist that through genetic engineering, it is no longer rapeseed, but “canola” instead.
According to Dr. Josh Axe, “It’s an industrial oil, not a food, and has been used in candles, soaps, lipsticks, lubricants, inks and biofuels. Rapeseed oil is what is used to make mustard gas. In its natural state, it causes respiratory distress, constipation, emphysema, anemia, irritability and blindness.”