Kauffman & Associates, Inc., an American Indian-owned communications and professional services firm, has won the 2014 National Health Information Award for its 2-year national campaign encouraging American Indians and Alaska Natives to sign up for health insurance under the Affordable Care Act. Other 2014 award winners include the American Association of Retired Persons, American Lung Association, Parents Magazine and the Mayo Clinic. The National Health Information Awards program honors high-quality consumer health information. The awards program is organized by the Health Information Resource Center, a national clearinghouse for consumer health professionals who work in consumer health education fields.
Working with its client, the Centers for Medicare and Medicaid Services’ (CMS) Tribal Affairs Group, KAI tested messages and images with American Indian and Alaska Native stakeholders throughout the United States and created radio spots, videos, billboards, bus signs, brochures, fact sheets and social media spots. KAI also recruited partner organizations from across the country and conducted outreach at large powwows, conferences, summits and sports events. KAI Vice President for Communications, Kim Blessing, reported “the campaign generated more than 100 million media impressions, recruited 113 tribal and organizational partners and distributed 23,000 informational brochures”.
“American Indian and Alaska Native people finally have the opportunity to ensure their health needs are fully covered, but they have to sign up. This is so important. It was a privilege to help CMS with this campaign,” said KAI President Jo Ann Kauffman, a public health professional and member of the Nez Perce Tribe.
The campaign also included a 7-minute video featuring former CBS News reporter Hattie Kauffman. This video, directed by Josephine Keefe, won the 2014 Telly Award earlier this year. The video is available online and is currently being played in Indian health clinic waiting rooms across the nation. Monthly radio public service announcements (PSA) were also produced by KAI, and featured both English and Native language speakers. Radio PSAs were sent to Native radios each month on topics about special benefits and protections for American Indians and Alaska Natives. These PSAs were recorded in English, Navajo, Lakota, Ojibwe and Yupik. Companion “drop-in” articles were placed in Native newspapers to reinforce the radio messages.
KAI has provided research and communications support to federal agencies, tribes, nonprofits and foundations in the area of public health, education, justice and community development since 1990.
“People die of cancer in Native American populations higher than other groups,” said Jani Ingram, associate professor of chemistry and biochemistry at NAU and member of the Navajo Nation.
According to the Intercultural Cancer Council, cancer is the third-leading cause of death among Native Americans, but there is no conclusive evidence to determine why.
Since 2002, NACP has worked to understand the reason cancer affects Native Americans, specifically tribes in the Southwest, at higher rates and seeks to engage Native American college students in entering science fields to help further research.
NAU’s program has 10 student researchers working under Ingram, some whom have been personally impacted by the deadly disease.
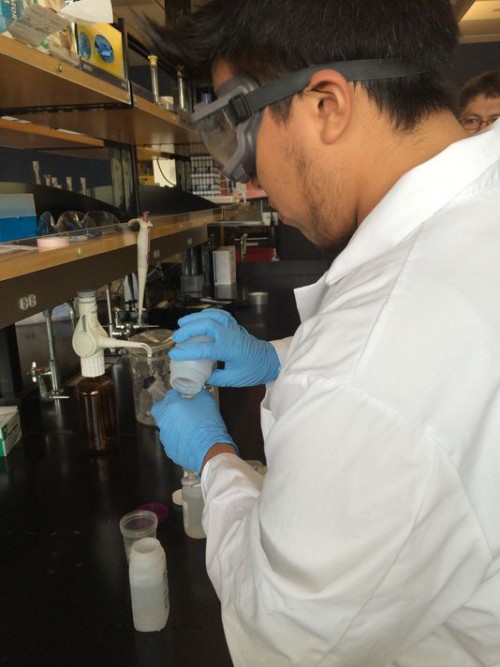
“It started with my grandfather, who worked in uranium mines and he died from lung cancer,” said NAU senior Erik Peaches, who is of Navajo descent.
Erik Peaches, NAU senior, works in lab as part of the Native American Cancer Prevention project at NAU.(Photo: 12 News)
In recent years, cancer spikes among older Navajos have been attributed to uranium exposure, a mining industry that boomed on the Navajo Reservation during the 1950s. The radioactive element still threatens communities surrounding abandoned mines and even contaminates drinking water.
NAU senior Ethan Paddock’s grandmother battled breast cancer that he says was caused by uranium exposure on the Navajo Nation.
“My family is from Cameron (Ariz.) and I know there is a huge uranium deposit over there,” Paddock said. “And it’s actually affected my grandmother and (she) got breast cancer.”
After a round of chemotherapy, Paddock’s grandmother has been declared cancer-free, but most with the disease don’t have the same outcome.
The grant money will continue the research being conducted in the Hopi, Navajo and Tohono O’odham communities, work that Ingram said more Native American students should consider.
“If it is a native student, a Navajo student, a Hopi student working on an issue that’s really important to their community, the passion is just right there,” Ingram said.
If you have ever attended a Native American PowWow you have probably noticed vendors selling a large doughy piece of bread called fry bread. Fry bread is an incredibly popular food, very much like an unsweetened funnel cake. American Indian fry bread might seem like a traditional food but it originated in a painful way. The most helpful hint that you can be given about Native American fry bread is to understand how and why this food came about. Native American fry bread may be a symbol of their culture. However, its beginning was steeped in tragedy.
History
Fry bread was first made approximately 144 years ago after the United States forced the Navajo to complete the “Long Walk,” which was a 300 mile walk where many people lost their lives. These Navajo people were moved to a land that was not fertile for traditional vegetables and beans. They were then forced to live on government canned goods: flour, sugar, salt, baking powder, powdered milk and lard. The Navajo people began using what they had and they created fry bread. Fry bread became a symbol of their survival and is always present at PowWows.
Ingredients
Fry bread is made from very simple ingredients. In order to make a dozen fry breads you will need: 2 cups sifted flour, 2 teaspoons baking powder, 1/2 teaspoon salt, 1 tablespoon shortening, approximately 1 cup water, and approximately one cup of oil. The recipe, as well as the style of cooking, has remain unchanged.
Preparation
First sift the flour, baking powder and salt together. Then add the shortening — a helpful hint is to use a pastry blender which will help incorporate the wet and dry ingredients. If you don’t have a pastry blender use butter knives. The next step is important, add just enough water to make a soft dough. If you add too much your dough won’t have the right consistency. Knead dough until smooth. Roll dough into small balls. Cover dough with a damp towel for ten minutes. Roll the ball in your hands until each ball flattens into a 4-inch round discs. It is important that you cook the dough in a skillet to keep the right texture of fry bread. Pour oil in the skillet and heat, ensure that you have at least an 1 inch of hot oil. Fry each round of dough until it becomes a light golden brown, turn it over once. The bread will puff up as it fries. Drain the fry bread on a paper towel when it’s done.
Serving
Fry bread is delicious by itself or you could serve it a multitude of ways. Drizzle the fry bread with a tiny bit of honey and powdered sugar or just add a little bit of jam. Many people cut a slit through the fry bread and stuff it with different foods including ground beef and beans. Another traditional recipe is the Indian Taco, the fry bread replaces the corn tortilla of a traditional taco. Fry bread is a very good bread but you should be mindful of what you are eating. Remember that this food is a story of resiliency and survival .
Public health officials in the Northwest say Ebola poses little threat to the region, but they are prepared to isolate and treat infected health workers or travelers. There have been no suspected or confirmed cases in Oregon or in Washington.
The Ebola virus. CDC
Oregon state Health Officer Katrina Hedberg says that most people traveling between West Africa and the United States are aware of the risk of Ebola.
“Most people, we hope ,will self identify, will want to get evaluated, will not want to spread any infection to other people,” she says.
Hedberg says emergency rooms and hospitals have been reminded to ask patients about recent travel. If you’ve been in West Africa and develop a fever or diarrhea, share your travel history with a doctor. Hedberg says standard isolation protocols hospitals use to treat patients with highly contagious diseases like the measles would be adequate for an Ebola patient as well.
Washington’s state public health laboratory is among relatively few in the US that the CDC has certified to test for Ebola.
Scott Lindquist, the state epidemiologist, says so far no tests have been requested.
Ebola has killed more than 2,000 people in West Africa, according to the World Health Organization.
Twenty-two tribes and indigenous organizations in 15 states will receive a total of copy1.3 million in grants from the Centers for Disease Control to combat chronic diseases commonly plaguing Indian country, the U.S. Department of Health and Human Services announced on September 25.
The biggest winner is the Alaska Native Tribal Health Consortium, which got copy.1 million, HHS said in a release. The smallest award went to Santa Ana Pueblo, for copy20,000.
It is part of overall grants totaling about $212 million awarded to all 50 states and the District of Columbia “to support programs aimed at preventing chronic diseases such as heart disease, stroke and diabetes,” the U.S. Department of Health and Human Services said in a statement. “This new initiative aims to prevent heart disease, diabetes, stroke, and associated risk factors in American Indian tribes and Alaska Native villages through a holistic approach to population health and wellness.”
These are all prevalent problems in Indian country.
The grantees will work within their communities using culturally appropriate measures to reduce exposure and use of commercial tobacco, improve nutrition and exercise, support breastfeeding, boost health literacy and strengthen team-based care by linking community resources with clinical services, HHS said. Half the awards are going directly to tribes, while the other half will be used to support tribal organizations that provide services, training, assistance and leadership in various areas to tribes and villages. The program is financed by the Prevention and Public Health Fund of the Affordable Care Act, HHS noted.
The other tribal grantees were the InterTribal Council of Arizona, Inc., which got $850,000; the California Rural Indian Health Board, Inc., whose grant was $788,972; United Indian Health Services, Inc., in California, with $650,000; the Nez Perce Tribe in Idaho, which is awarded $200,000; the Kickapoo Tribe in Kansas, with copy94,876; the Sault Sainte Marie Tribe of Chippewa Indians in Michigan, which gets $325,000; Fort Peck Community College in Montana, with $317,039; also in Montana, the Montana-Wyoming Tribal Leaders Council, which got $648,124; the Winnebago Tribe of Nebraska, netting copy78,493; the Albuquerque Area Indian Health Board, Inc. of New Mexico, which received $850,000; Oklahoma City Area Inter-Tribal Health Board, with $850,000; two grants in Oregon, with $850,000 going to the Northwest Portland Area Indian Health Board and copy99,159 to the Yellowhawk Tribal Health Center; the Catawba Indian Nation of South Carolina got copy99,804; the Great Plains Tribal Chairmen’s Health Board in South Dakota netted $650,000, while the Lower Brule Sioux Tribe received $200,000. In Tennessee the United South and Eastern Tribes, Inc. (USET) got $849,998, the Great Lakes Inter-Tribal Council, Inc. in Wisconsin received $850,000, and, also in Wisconsin, the Red Cliff Band of Lake Superior Chippewa Indians got $200,000.
SEATTLE – The patient care team at ACCES (A BluePearl Veterinary Partners) specialty and emergency hospital for pets in Seattle and Renton is encouraging pet parents to include their pets when making family disaster plans. The Federal Emergency Management Agency (FEMA) is sponsoring America’s PrepareAthon! on Sept. 30, as part of the federal government’s National Preparedness Month. The event is meant to motivate individuals, organizations and communities to prepare in advance for natural disasters like earthquakes, floods, hurricanes, tornados, wildfires and winter storms.
“Disasters can happen with little notice and be devastating. But being prepared can save your life or that of your family members — including your pets, ” said Amanda McNabb, emergency clinician with ACCES in Seattle, Washington, and a member of the WSDA Reserve Veterinary Corps. “That’s why we strongly recommend pets be included in your disaster preparedness plan.”
Here are some tips recommended by the ACCES team:
CREATE AN EMERGENCY KIT FOR YOUR PET BEFORE A DISASTER
Keep current documentation of your pet’s medical records and vaccination history in the emergency kit.
Include your pet’s license information.
Have a current photograph of your pet in the kit.
Keep a checklist in the kit of items to pull together when a disaster is imminent, including these:Have an evacuation strategy: Have a list including addresses and phone numbers of specialized pet shelters, animal control shelters, veterinary clinics, and friends and relatives out of harm’s way who are potential refuges for your pet during a disaster. Familiarize yourself with the location of each so if you need to evacuate, you can plan your route accordingly.
Collar: Make sure your pet’s collar has an identification tag with your contact information.
Leash: Use a leash if you evacuate or bring your pet to a shelter because pets can become easily disoriented if they slip away from you.
Carrier: Have a properly sized pet carrier for each animal handy. Carriers should be large enough for the animal to stand and turn around.
Medications: Have a two-week supply of medications and care instructions to bring with you.
Food: A two-week supply of food should always be kept on-hand in case of an emergency.
Other: Make a list of other items to add at the last minute such as food, bowls, can opener, cat litter, water and cleaning supplies.
DURING A DISASTER
Gather together in one place all items on your pet’s emergency checklist. A laundry basket is easy to carry and a good size for this purpose.
Animals brought to a pet shelter may be required to have any or all of the following:Pet shelters will be filled on first come, first-served basis. Call ahead and determine availability.
Leash and collar with identification tag
Rabies tag
Identification on all belongings
Suitable carrier or cage
Ample supply of food, water and food bowls
Necessary medications and specific, written care instructions
Newspapers, trash bags and other supplies for clean-up
Bring pets indoors well in advance of a storm. Reassure and calm them throughout.
Monitor your pets’ behavior, because animals can become defensive or aggressive due to the stress of the situation.
AFTER A DISASTER
Walk pets on leashes until they become re-oriented to the area. Familiar scents and landmarks may be altered and pets could easily be confused and become lost. Also, downed power lines, debris, snakes and other critters brought in with high water can all pose a threat for animals after a disaster.
If your pet is lost during a disaster, contact your local animal control office to find out where lost animals are being housed. Bring along the picture of your pet and information about the microchip.
About Us: ACCES (A BluePearl Veterinary Partners Hospital) serves the Puget Sound region by offering the highest quality specialty, critical care, emergency medicine and specialty services to veterinarians and their clients 24-hours a day/365 days a year at locations in Seattle and Renton. For more information on ACCES, please visit criticalcarevets.com.
BluePearl Veterinary Partners employs 1,800 team members including more than 450 veterinarians. BluePearl hospitals offer referral-only, specialty care services and most offer 24-hour emergency care. BluePearl does not provide primary care. The company is one of the world’s principal providers of approved veterinary residency and internship programs. BluePearl also participates in clinical trials that investigate the effectiveness of new veterinary drugs and treatments, providing pet families access to cutting-edge medicine that is not yet commercially available. BluePearl is headquartered in Tampa, Fla. For more information on BluePearl Veterinary Partners, please visit bluepearlvet.com.
Once again, the federal government is funding “navigators” in Montana to help the uninsured buy private, subsidized health coverage this fall — with a new emphasis on Native American consumers.
Earlier this month, federal officials awarded $609,000 in navigator grants to three Montana groups: Planned Parenthood of Montana, the Montana Health Network and the Montana Wyoming Tribal Leaders Council.
“We had great, great success with the program last year,” Martha Stahl, CEO of Planned Parenthood of Montana, said Monday. “I think it’s a great way to continue our mission of connecting people with affordable health care, which is what we’re all about.”
Stahl said her group will be working closely with the other two grant recipients and other organizations to sign up more people for health insurance under the Affordable Care Act, as well as target Native Americans. Planned Parenthood and the Health Network had navigator programs last year.
Navigators, who must be certified by the state insurance commissioner, help people buy private health insurance through the online “marketplace,” a key part of the ACA, the federal health-care overhaul also known as “Obamacare.”
Individuals buying policies on the marketplace can get federal subsidies to offset the cost of those policies. Lower-income consumers also can get further discounts on certain marketplace policies.
Most consumers who earn less than 400 percent of the federal poverty level — about $79,000 for a family of three — are eligible for the subsidies, which are paid directly to the insurance company.
The Obama administration launched the marketplaces last October in 34 states, including Montana, initially with disastrous results. Beset with technical problems, the marketplaces barely worked.
However, by the end of March, more than 36,000 Montanans gained coverage through marketplace policies, out of 8 million people nationwide.
The marketplaces will open again this year Nov. 15. Customers can shop for and purchase new policies for 2015. Four companies will be offering policies on Montana’s marketplace.
Cheryl Belcourt, executive director of the Montana-Wyoming Tribal Leaders Council in Billings, said the group will use its $142,000 grant to hire some navigators and coordinate with other groups to encourage Native Americans both on and off reservations to buy marketplace policies.
Many Native Americans think the policies are not for them, because they expect to use the Indian Health Service and don’t face a tax penalty if they’re not insured, Belcourt said.
However, the affordable private policies and their low-cost coverage can expand health care for Native Americans, she said.
“This is an opportunity to address the health disparities of Native American people,” Belcourt said. “We want to be able to really make a difference in terms of the quality of life for Indian people.”
Chris Hopkins of the Montana Health Network, a consortium of smaller hospitals and health-care centers, said its $175,000 grant will be used to add nine new navigators to the 20 it already trained with last year’s grant. Most of them are staffers at hospitals and nursing homes.
“Our focus is to have local people providing services in their own community, rather than having someone come in from the outside, do a presentation, and then leave,” he said.
The Montana Primary Care Association, which represents federally funded health clinics, had a navigator program last year but did not get a grant this year.
Amanda Harrow of the association said clinics will continue to work with various groups to help people sign up for ACA-subsidized policies.
Health and Human Services Secretary Sylvia M. Burwell announced last week that individuals eligible to receive health care from an Indian Health Service (IHS), tribal, or urban Indian health program provider are now able to claim an exemption from the shared responsibility payment through the tax filing process starting with the 2014 tax year. This benefit was previously only available to members of federally recognized tribes (including Alaska Native shareholders). American Indian and Alaska Native individuals will continue to have the option of submitting the exemption application through the Health Insurance Marketplace.
Prior to this week’s announcement, only individuals who were members of a federally recognized tribe were able to claim an exemption through the federal tax filing process. Individuals who are eligible to receive services from an Indian health care provider are eligible for a separate hardship exemption but were required to obtain this exemption through the Health Insurance Marketplace by filing a paper application.
The availability of the online tax filing process to apply for the hardship exemption will save time and reduce duplication of effort. Qualification for the Indian exemption can be established by attestation of membership in a federally recognized tribe or eligibility to receive services from an Indian health care provider.
Secretary Burwell first announced this updated rule at the Secretary’s Tribal Advisory Committee meeting on September 18, 2014. This benefit of claiming the exemption through the tax filing process was initiated based on requests by tribal leaders. The IHS worked closely with the Centers for Medicare and Medicaid Services and the Internal Revenue Service to extend these options to individuals eligible to receive services from an Indian health care provider.
The IHS, an agency in the U.S. Department of Health and Human Services, provides a comprehensive health service delivery system for approximately 2.2 million American Indians and Alaska Natives who are members of federally recognized tribes.
PORT TOWNSEND — Lethal levels of marine biotoxins that cause paralytic shellfish poisoning have been detected in shellfish taken from Quilcene Bay, Jefferson County health officials warned Monday.
Quilcene and Dabob bays have been closed to the recreational harvest of molluscan shellfish — clams, oysters, mussels and scallops — since Sept. 8.
Paralytic shellfish poisoning, or PSP, concentrations have risen to more than 6,000 micrograms per 100 grams of shellfish.
That’s 75 times the 80-microgram closure level, and twice the levels detected last week.
“It keeps climbing,” said Michael Dawson, water quality lead for Jefferson County Environmental Health.
A combination of warm weather and calm water may be contributing to the elevated levels of PSP, Dawson said
Additional samples from Quilcene Bay and surrounding areas were collected Monday.
“Right now, we’re mostly wanting to check and see if it might be spreading,” Dawson said.
“So we’ve been checking down the Hood Canal.”
The state Department of Health is warning the public that eating shellfish with such high amounts of toxin is potentially deadly.
Symptoms of PSP can appear within minutes and usually begins with tingling lips and tongue moving to the hands and feet, followed by difficulty breathing and potentially death.
Danger signs have been posted at public beaches warning the public not to eat the shellfish, Dawson said.
Marine biotoxins are not destroyed by cooking or freezing.
The closure does not apply to shrimp.
Crabmeat is not known to contain the biotoxin, but the guts can contain unsafe levels.
To be safe, clean crab thoroughly and discard the guts, health officials say.
Commercially-harvested shellfish are tested for toxins prior to distribution and should be safe to eat.
Areas closed to the recreational harvest of all species of shellfish in Jefferson County are Quilcene Bay, Dabob Bay and Discovery Bay.
Kilisut Harbor, including Mystery Bay, and the Port Ludlow area are closed to the recreational harvest of butter and varnish clams only.
Jefferson County Public Health will continue to test affected beaches and will notify the public when shellfish are safe to harvest, officials said.
In Clallam County, the recreational harvest of butter clams is closed from Cape Flattery to Dungeness Spit.
Varnish clams are closed along the entire North Olympic Peninsula.
Sequim Bay is closed to all species of shellfish.
Seasonal closures are in effect for the Pacific Ocean beaches.
Recreational shellfish harvesters can get the latest information about the safety of shellfish on the state website at www.doh.wa.gov or by phoning 800-562-5632 before harvesting shellfish anywhere in the state.
Recreational shellfishers also should consult state Fish and Wildlife at www.wdfw.wa.gov.
Pam James, co-founder of Native Strategies Photo/Shannon Kissinger
By Kyle Taylor Lucas, Tulalip News
This is the second story in a series on the intersection of chronic health and addiction issues and Adverse Childhood Experiences (ACEs among American Indians. The series focuses upon contributing factors of high ACE numbers and substance abuse and behavioral and health disparities in American Indians.
The ACEs Study became a reality due to a breakthrough from an unexpected source—an obesity clinic led in 1985 by Dr. Vincent Felitti, chief of Kaiser Permanente’s Department of Preventive Medicine, San Diego. Dr. Felitti was shocked when more than fifty percent of his patients dropped out of the study despite their desperate desire to lose weight. His refusal to give up on them led to individual interviews where he learned that a majority had experienced childhood sexual trauma. That led to a 25-year research project by the Centers for Disease Control and Prevention (CDC) and Kaiser Permanente. The landmark study linked childhood adversity to major chronic illness, social problems, and early death.
According to the CDC, “the Adverse Childhood Experiences (ACE) Study is one of the largest investigations ever conducted to assess associations between childhood maltreatment and later-life health and well-being.” The study included more than 17,000 Health Maintenance Organization members who in routine physicals provided detailed information about childhood experiences of abuse, neglect, and family dysfunction. The ACEs Study links childhood trauma to social and emotional problems as well as chronic adult diseases such as disease, diabetes, depression, violence, being a victim of violence, and suicide.
Since the ACEs Study, hundreds of published scientific articles, workshops, and conferences have helped practitioners better understand the importance of reducing childhood adversity to overcome myriad social and health issues facing American society. See the ACEs questionnaire, here: http://www.acestudy.org/files/ACE_Score_Calculator.pdf. Learn more about the ACEs Study here: http://www.cdc.gov/violenceprevention/acestudy/
The ACEs research is of significant relevance to American Indian/Alaska Native (AIAN) communities beset with behavioral and physical health issues—disproportionately high as compared to the general population.
Unquestionably, any discussion of social and health disparities in Indian Country must include historic trauma, and the political and economic realities affecting American Indians and tribes. Research into epigenetics subsequent to the original ACEs Study indicates that historic trauma is likely one of the primary contributors to disparate behavioral and physical health issues affecting AIANs. Subsequent stories will more fully explore the physiological brain changes that result from childhood adversity.
Native Strategies – Addressing Historic Trauma in Native Communities
Tribal experts in the area of historic trauma emphasize that while the ACEs Study is important, it is also important to ensure concurrent address of historical trauma on AIANs and tribal communities.
One of those experts is Pam James who is co-founder of Native Strategies, a non-profit organization established with her husband and partner, Gordon James, in 2009. Pam is a member of the Colville Confederated Tribes and Gordon is a Skokomish Tribal member. The two have been consulting on historic trauma and Native wellness in tribal communities for the past thirty years. Pam earned a B.A. Degree in Psychology and Native American Studies from The Evergreen State College and a BHA in community health from the University of Washington.
“Until we established our non-profit, we did freelance consulting. We worked with the Native Wellness organization, sought grant funding, and wrote a wellness book. Then we used our book to write a curriculum that we’ve applied in our work,” said James.
The non-profit allows better access to funding and resources to further their work empowering tribal people and communities. “We are able to provide training and technical assistance absent tribal politics,” said James who noted they are also free to be creative in designing a broad array of programs, training, services, and technical assistance. “We’ve helped several organizations start their own non-profits. We do a lot of grant writing. We do workshops around historical trauma, parenting, healthy relationships, and government-to-government training. We also do planning and program evaluations and help organizations get into compliance.”
James said one of the most sensitive and impactful of their workshops is healthy workplace training. “We look at it holistically, at interpersonal relationships, family relationships, and relationships to all things–earth and to all creation.” She asks, “How do you create a healthy workplace? You can’t do that until you begin to address the historic trauma.” In their work, James said they help to rewire the brain for positive impact, noting, “Behavior is just a habit. We have to change the habit. I do it from a cultural perspective and I blend in humor.”
However, James is mindful of her approach. She said, “every workshop, every training I do, people get triggered,” so she is careful with her audience. They try to unlearn negative behaviors. In the communities, she finds, “Though it doesn’t work, people do the same thing over and over again expecting a different result.” She said their training “takes people back to that value system that our people always had, treating people with honor and respect. We have a roadmap that asks, “What do you want in your life, spiritually, emotionally, and how do you start creating the life you want?”” She said repetitiveness in practice and training is critical and noted the impossibility of creating change in a workshop or two.
Asked whether training the trainer is part of their work, James replied that it was and that it is essential. “We help train the trainer for tribes so that they can teach it themselves. First, we do community training, then a three-day “train the trainer” workshop, and then we come back in 3-6 months to assist them with their first training. It’s very sensitive. What do you do when someone gets triggered? We help to prepare them.”
About their generational trauma and wellness work, James added, “In our training, we’re opening awareness. The second step is intervention. How do we implement and make change? The third step is continuing education and putting it into practice. It is developing new ways of coping, replacing behaviors, and doing it on a consistent basis. It’s a theory and it’s ongoing.”
However, she said, “Most of our tribal communities are in crisis mode by the time they call. I urge them to call us before that.” She noted three stages—prevention, emergent, and intervention. “I urge them to look at those areas and ask, “How do we get to the place where we’re doing prevention rather than intervention?” Tribes have to start looking at this type of training as ongoing. Just like computer classes. This is not a one-time shot.”
In their training, James said they often support eight-week parenting classes. However, she recommends to clients, “Before we do that, let’s do a healthy relationship class!” Again, she says it is a matter of steps, mentally, emotionally, and educationally. “First of all, we start with the parents to help them learn how to interact with each other. We are in a society that wants a quick fix, but there is no quick fix. It’s about awareness, learning new skills and behaviors, and then we have to practice, practice, practice. It’s not about the end result it’s the journey.”
James said she attended one of Laura Porter’s workshops on ACEs and thought, “Wow, this would have been great to know years ago! Oh my gosh, I wish we had been involved.” To date, only a few tribes have engaged with the state’s research work around the CDC ACEs Study and measurements. James believes “ACEs is one piece of the puzzle, one piece of the process for Native people.” She said her non-profit is looking at funding opportunities to develop a curricula based on their 30 years of work. They plan to work with an advisory team of Native people and the curricula will be designed for implementation by tribal communities, and culturally appropriate to their needs.
Specific to generational historic trauma, James believes “The ACEs information doesn’t go far enough. The State is a very good example of a sense of guilt. They don’t really want to acknowledge it. It’s painful to acknowledge what was done to Native people. There is a lot of effort being made to change it, but it’s still there.”
ACEs and Physiological Rewiring of the Developing Brain
Asked about her knowledge of current scientific research on the relationship of childhood adversity and epigenetics—the study of physiological brain changes and potential application to the study of historic trauma in Native communities, James becomes animated. She noted a weeklong workshop she attended with Dr. Bruce Perry, the author of “The Boy Who was Raised as a Dog” and “Born for Love.” She said, “What an amazing man. His focus has been trauma.” She said he validated the tribal community’s long assertions of unresolved multigenerational trauma, and that the brain is actually hard-wired for empathy, but things happen to the brain when babies and children experience adversity and trauma.
James discussed the work of Dr. Patricia K. Kuhl who of the University of Washington, whose trainings she has attended. She co-authored the book, “The Scientist in the Crib.”
At one workshop, Dr. Kuhl presented studies of two children’s brains from newborn to age three–one child from a happy home and the other from a neglected home. They conducted CAT scans at ages 3, 6, and 9 months. At the beginning, their brains were identical, but by the time they were nine months old, the brain of the neglected child was visibly shrinking. Considered in the context of social and health disparities and life chances for AIANs, this is quite remarkable. The above study demonstrated that disparities begin in the crib, but as the ACEs Study and ensuing research has shown, it is intergenerational, and even in the womb. If the mother and father have high ACE scores based upon their own childhood adversity, the children are also likely to have high ACE scores unless there is intervention.
James is optimistic. She said that although the research shows adversity is generational, “It also validates that we can reverse it. It doesn’t have to be permanent. Some of it might be, but we can reverse much of it. Our ancestors adapted. We learned how to adapt for our environment; it is human nature to survive. Those are the pieces that are not happening in our community.”
Family and Community Roles and Traditions
Lamenting the negative impacts of technology, James said, “Televisions, iPads, Xboxes are the babysitters of today. They are impacting how our children develop, how their brains develop. Technology has disconnected us as people.” She grew up in Inchelium where they did not have a telephone until 1978. “All the grandmothers and everyone would come together, bring old clothes, and make quilts. They lined them with old army blankets. There was a spiritual part of that. Every newborn received a quilt. We’re not doing those kinds of activities that inspire and help our children to learn about community.” James is concerned that technology today limits human contact important to a sense of being part of something greater and of the responsibility accompanying it.
Another significant hurdle is overcoming the lateral violence that is a symptom of ACEs. James said that in her counseling work, she discovered, “We get addicted to pity, to negativity, and we become chaos junkies.” She believes people have forgotten about how just to be. “The Vision Quest taught us how to be alone, to be one with nature, to be alone physically and mentally. It taught us how to control our mind, our spirit, and our bodies.” She thinks some of those teachings can be built into the curricula to teach people how to, again, “sit quietly with themselves, to sit and listen.”
Applying the ACEs Study and Measurements to Native Wellness
James’ family of origin was not unlike many Native homes. She and her eight brothers and sisters grew up with domestic violence, alcoholism, and physical and sexual abuse. She began doing this work in 1986 when the Seattle Indian Health Board received a federal grant to put together a curriculum. She was among 40 chosen from different tribes to participate in a two-week intensive training that was life changing for her. “They stripped us spiritually and emotionally. We had to address our own trauma. We could not help others until we worked on ourselves and healed ourselves. There was no college that could give me what that training did!”
In the training, Jane Middelton-Moz, an internationally known speaker and author with decades of experience in childhood trauma and community intervention took part in the training. She addressed the pain of adult children of alcoholics (ACoA), a topic about which she has written extensively. “It was basically an ACE’s study done with Native people and it was all about the trauma.” James recounted Middleton-Moz’s journey to Germany where she worked with holocaust survivors and her later study of American Indian tribes. She discovered that they had developed the same trauma characteristics. “She was a psychotherapist and I felt blessed to have the opportunity to be mentored by her.” James noted that their work has essentially taken Middleton-Moz’s study of ACoA and applied it to multi-generational trauma among tribal communities.
Asked how the new research on childhood adversity can help Native communities, James said, “The ACEs Study is good in that it gives us the validation and affirms what we’ve known. This is what has been happening in our communities for hundreds of years.” She noted the mental and physical health issues evidenced by high juvenile suicide rates, 638 percent higher incidence of alcoholism than the general population, addiction, and disparate social, and health issues in Indian Country are all traceable to generational trauma and adverse childhood experiences.
However, James believes the survey mechanisms must be appropriate. She said, “The reality is that a lot of times when so-called experts go in and do the surveys, the tribal members don’t tell the whole truth.” Tribal communities are tight-knit and everyone knows everyone and their business. It may be that a special survey mechanism is necessary for tribal communities. James said, “It will be difficult to get reliable data if the members don’t trust enough to give accurate information, to tell the whole truth.”
Those involved in tribal wellness have said for years, and James echoes this, that it is important to put the disparate social and health issues in Indian Country into context. “We have people who have suffered such trauma in their lifetimes, in their parents, and grandparent’s lives!” said James.
People forget that generations of American Indians experienced breaks in the family unit caused by the government’s forcible removal of children placed into Indian boarding schools. Indian children were deprived of parental nurturing; many were physically and sexually abused. They did not learn how to parent and nurture their children, but at adulthood, they were returned to the reservation to start their own families and the same cycle was repeated.
In their workshops, James stresses traditions. “We’ve adopted behaviors that were not ours traditionally. Instead, we go back to the medicine wheel, it teaches you everything—body and mind. When you look at what is happening with our communities, we’ve lost touch with all of the ceremonies, languages, and the practices that kept us resilient. There is a veneer of positivity, but underneath there’s all this pain.”
Clearly passionate about her work, James makes the call, “Someone has to be the voice of our children, someone has to stand up and take the arrows, stand up and say this is not what our ancestors wanted. I really believe this is the core work if we can get it into our communities, we’re going to change, and it has to take place for our survival.”
Integration of ACEs Research in Tribal Family Services and Other Programs
As Sherry Guzman, Mental Health Manager in the Tulalip Family Services Department said, about the ACEs Study, “Most tribes were very leery at first, but I went forward with it because I saw the value of it. It enabled me to see the difference in average of Washington State versus Tulalip Tribes. I like the ACEs model because it gives a base to compare something to.” She, too, felt the ACEs measurements validated what she and others in Indian Country have advocated—that unresolved generational trauma is a significant contributor to social and health disparities among tribes.
Guzman’s department has scheduled an all-staff meeting focused upon the ACEs Study and Tulalip’s work with the statewide network a few years ago. They hope to re-establish a dialogue and consider the future direction the Tribe may take in applying the ACEs Study and measurements in its programs.
In communities utilizing the ACEs measurement across the nation, the subsequent application of community resilience building has consistently demonstrated success in lowering of ACE scores in community members, which in turn helps build stronger and more resilient communities. Imagine the possibilities if communities invested in families on the front end, supporting pre-natal work, pre-school and all day kindergarten, rather than building juvenile detention centers and adult prisons.
At least twenty-one states have communities actively engaged in ACEs work.
Future stories in this series look at that work and new developments in ACEs research, including neurobiology, epigenetics, and the developing brain. Also featured will be tribal organizations applying similar intervention and measurements to address generational trauma. Because ACEs extend beyond the nuclear family to educational and child welfare policies, and to racism in social, police, courts, and other institutions controlling the lives of Indians, those intersections are reviewed along with the economics. Finally, the series will explore the potential of ACEs measurement in prevention and for building resiliency for American Indian people and tribes.
Kyle Taylor Lucas is a freelance journalist and speaker. She is a member of The Tulalip Tribes and can be reached at KyleTaylorLucas@msn.com / Linkedin: http://www.linkedin.com/in/kyletaylorlucas / 360.259.0535 cell

 Kauffman & Associates, Inc., an American Indian-owned communications and professional services firm, has won the 2014 National Health Information Award for its 2-year national campaign encouraging American Indians and Alaska Natives to sign up for health insurance under the Affordable Care Act. Other 2014 award winners include the American Association of Retired Persons, American Lung Association, Parents Magazine and the Mayo Clinic. The National Health Information Awards program honors high-quality consumer health information. The awards program is organized by the Health Information Resource Center, a national clearinghouse for consumer health professionals who work in consumer health education fields.
Kauffman & Associates, Inc., an American Indian-owned communications and professional services firm, has won the 2014 National Health Information Award for its 2-year national campaign encouraging American Indians and Alaska Natives to sign up for health insurance under the Affordable Care Act. Other 2014 award winners include the American Association of Retired Persons, American Lung Association, Parents Magazine and the Mayo Clinic. The National Health Information Awards program honors high-quality consumer health information. The awards program is organized by the Health Information Resource Center, a national clearinghouse for consumer health professionals who work in consumer health education fields.